
What is Gilchrist Blastomycosis?
Gilchrist blastomycosis, or North American blastomycosis (Gilch-rist disease, Chicago disease – English; Blastomykose – German; blastomycose – French; blastomicosis – Spanish) – a chronic disease related to deep mycosis, characterized by the formation of granulomas and purulent processes in the lungs , skin, subcutaneous tissue, and during dissemination – in many internal organs.
Causes of Gilchrist Blastomycosis
Pathogen – Blastomyces dermalitidis is among the biphasic fungi. In the tissues, it has the form of round yeast cells with a diameter of 8–15 μm, white colonies, later of brownish color, consisting mainly of mycelium filaments, form on the Saburo nutrient medium.
In the tissues only the yeast phase of the fungus is observed. When cultivated on fresh medium at a temperature of 37 ° C, the mycelial phase can pass into the yeast phase, and at a temperature below 30 ° C, it again goes into the mycelial phase. Under natural conditions, this type of fungus is found in dogs and horses. From laboratory animals white mice are sensitive to blastomycosis.
Sources and routes of transmission are not well understood. The pathogen was found in the soil, in the mud. Epidemic outbreaks among people and animals (dogs) associated with being on the banks of small rivers in a wooded area are described. Reliable cases of transmission from person to person or from animal to person are not described. During epidemic outbreaks mostly children fell ill. There is no data on the increased incidence of persons with immunodeficiency. Usually, those with a normal immune system got sick. The disease was more often observed in the USA, sporadic cases were registered in Canada, Australia, India, France, Italy, Hungary, isolated cases were also observed in Russia.
Pathogenesis during Gilchrist Blastomycosis
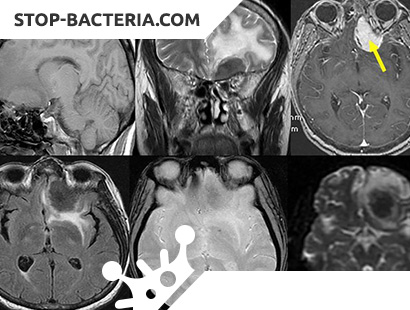
The gateway of infection is probably the respiratory tract, as evidenced by the primary lesions of the respiratory system. Skin lesions, which are also often seen in patients, are secondary as a result of the infection being carried from the lungs (localized mainly in closed areas of the skin). When the infection is generalized, the pathogen from the lungs gets into various organs (bones, liver, spleen, central nervous system). As a result of the infection, an allergic alteration develops. Transferred blastomycosis leaves a long and lasting immunity. In some infected (about 50%) blastomycosis is asymptomatic.
Symptoms of Gilchrist Blastomycosis
The incubation period ranges from 1 week to 4 months. In the clinical picture of blastomycosis, the main manifestations are lesion of the lungs and papillomatous ulcerative blastomycosis of the skin. Skin lesions usually develop on the background of pulmonary changes, the latter are observed in almost all patients, whereas skin changes may be absent. The pulmonary form of blastomycosis can begin gradually as a primary chronic, without severe acute phase of the disease. There is a general weakness, cough, body temperature rises, but only in some (about 20%) it exceeds 38 ° C, body weight decreases (in 40%), chest pains are frequent, shortness of breath. The admixture of blood in the sputum is observed in 30% of patients. Dry and wet rales are heard. Pleural friction noise is noted only in individual patients (10%). Some patients may have generalized lymphadenopathy, enlarged liver and spleen. Typical skin lesions are observed in 30-80% of patients.
Much less often (in 20-25% of patients) the pulmonary form of blastomycosis begins acutely, occurs with severe fever in all patients, and in 80-85% it rises above 38 ° C. Almost all patients have a strong cough, chest pain, dry and moist rales are heard. Often there is an admixture of blood in the sputum. This form is not characterized by an increase in the liver and spleen, skin lesions, and there is no pleural friction noise. The process is limited in this stage by the lungs.
Radiographically marked changes in the lymph nodes of the mediastinum, focal infiltrates, in some of them develop cavities with irregular contours. With dissemination, many organs are captured; these forms often end in the death of the patient.
A skin lesion begins with the appearance of a subcutaneous nodule, in place of which a papule forms, then a vesicle, a pustule, which turns into an ulcer. Papillomatous growths with small pustules and crusts form on the ulcer surface. The size of the skin lesions is gradually increasing, reaching 2-3 cm in diameter. They can be localized on any part of the skin (usually on the arms, legs, face, buttocks). At the site of injury, a thin, soft scar is formed during healing.
Complications – arthritis, osteomyelitis, brain damage (meningitis, brain abscess).
Diagnosing Gilchrist Blastomycosis
It is necessary to differentiate from other long-term lung diseases (tuberculosis, pulmonary forms of aspergillosis, nocardiosis, histoplasmosis, lung abscesses, neoplasms). Of great diagnostic importance is the characteristic skin lesion. To confirm the diagnosis using laboratory methods to detect the pathogen or antibodies to it. The pathogen can be isolated from the pus of skin lesions, pieces of biopsy tissue, sputum. To obtain a culture, crops are made on blood agar and Saburo medium. For the detection of antibodies, various reactions are used (CSC, REMA, blastotransformation reaction with a specific antigen, etc.).
Treatment of Gilchrist Blastomycosis
Acute forms of pulmonary blastomycosis can result in recovery without the use of anti-mycotic drugs. Chronic pulmonary forms, and especially disseminated, require long-term treatment. In these cases, amphotericin B is prescribed, as with aspergillosis. In recent years, recommending the use of a foreign drug – ketoconazole (Ketoconazole), which is used for long courses. When using relatively small doses of mg / day, adverse reactions were rarely observed, good results were obtained, but in some patients (about 10%) the disease recurred. At a dose of 800 mg / day, adverse reactions were often noted, but complete recovery occurred. With brain damage, the drug is ineffective.
The prognosis for disseminated forms without treatment almost all patients die. For other forms, the prognosis is more favorable.
Prevention of Gilchrist Blastomycosis
Prevention and activities in the outbreak are not developed.