
Diagnosis of Meningococcal Infection
Early diagnosis of meningococcal infection in children is important due to the rapidly progressing course, as well as the potentially fatal outcome. Actively identifying and accounting for the early symptoms of infection can increase the effectiveness of its diagnosis at the stage of first aid, which will speed up the flow of patients to the hospital.
The time window for diagnosing MI in children is extremely narrow. So, during the first 4-6 hours, most patients do not have specific symptoms, while after 24 hours the infection process becomes life-threatening. It was noted that in most children there was an early (on average 8 hours) onset of symptoms of hemodynamic disturbance – cooling hands and feet, discoloration of the skin. At the same time, the classic symptoms of meningococcal infection (meningism syndrome, hemorrhagic rash, impaired consciousness) developed much later, on average after 13-22 hours.
A general practitioner should diagnose meningococcemia as soon as possible only on the basis of supporting clinical signs: acute onset, fever, hemorrhagic rash.
It should be remembered that for a patient, overdiagnosis is better than an untimely diagnosis. It is also necessary to responsibly treat the diagnosis of meningitis, which is established clinically, in the presence of even moderately expressed cerebral and meningeal syndromes that occur against the background of fever and intoxication.
Specific laboratory diagnosis of meningococcal infection consists of bacteriological and serological studies.
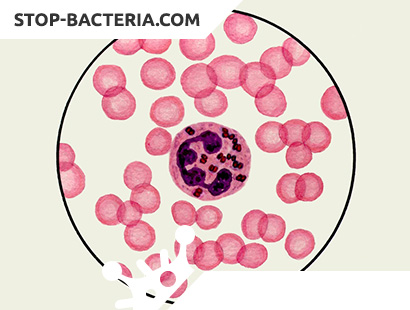
The material for bacteriological research is nasopharyngeal mucus, blood, cerebrospinal fluid. Outpatient can be carried out only sowing mucus from the nasopharynx. It must be remembered that the smear is taken with a sterile swab on a curved wire, preferably in the morning, until the patient brushed his teeth, rinsed his mouth, and ate. In the hospital, a bacteriological study of blood, cerebrospinal fluid, nasopharyngeal mucus is performed. From serological methods, RPHA and WIEF are used. As an express method, bacterioscopy of cerebrospinal fluid and blood (“thick drop”) is used, in which paired cocci stained negatively by Gram can be found mainly inside neutrophils. However, this method is indicative. In the peripheral blood of patients with a generalized form of the disease, hyperleukocytosis, elevated ESR, a sharp shift of the leukocyte formula to the left are noted. To diagnose meningitis, a lumbar puncture is necessary. With purulent meningitis, cerebrospinal fluid flows under high pressure (frequent drops, sometimes with a stream), cloudy, whitish. With late admission – greenish, viscous.
Differential diagnosis
The prodromal rash in the early period of meningococcemia, as mentioned above, is often interpreted as a manifestation of drug allergy. It is its rapid variability, disappearance in a short time with the greatest probability that can indicate a meningococcal etiology. Prodromal rash may resemble measles. But measles rash appears on the 4th-5th day from the onset of the catarrhal period. At the same time, in the catarrhal period of measles, scleritis, conjunctivitis, photophobia are observed, and a barking cough is disturbing. The first elements of a rash with measles appear on the face, an enanthema appears in the soft palate at the same time. In the future, the rash spreads over the body in a descending manner, has a drainage character.
Rash with infectious mononucleosis is core-like. The disease is preceded by tonsillitis, an increase in the cervical and other groups of lymph nodes. There is hepatolienal syndrome. Atypical mononuclear cells (virocytes) are detected in a general blood test.
A typical rash with scarlet fever is not similar to a rash with meningococcemia, however, accompanied by the appearance of a hemorrhagic component, it can cause doubts. Scarlet rash is located on the flexion surfaces of the limbs on a hyperemic skin background, concentrating in natural folds. There are typical changes in the mucous membranes: a “flaming” pharynx, tonsillitis, a “raspberry” tongue (its papillary structure is expressed).
A rash with hemorrhagic vasculitis often occurs after an acute respiratory infection. In this case, the child is in satisfactory condition, the temperature is normal. Elements of the rash are located symmetrically, more often on the skin of the extensor surfaces, in the ankle joints, on the buttocks.
In thrombocytopenic purpura, a rash from small petechiae to large ecchymoses is located on parts of the body that are often traumatized, and there may be hemorrhages on the mucous membranes of the mouth. Bleeding is characteristic. The general condition suffers little. Fever is not characteristic. In the peripheral blood, the platelet count is sharply reduced, the bleeding time is prolonged.
Treating Meningococcal Infection
Treatment should be started immediately.
First aid should be provided to the patient by the doctor who first suspected or diagnosed meningococcemia.
The patient is required to administer chloramphenicol succinate 25 mg / kg IU (single dose) + prednisone 2-Z mg / kg. Intravenous administration of these drugs is preferable, since intramuscular administration of antibiotics and hormones is not effective if microcirculation is disturbed. If there are signs of ITS, the main treatment is the use of massive doses of corticosteroids from 5 to 20 mg / kg, replenishment of the volume of circulating blood (administration of drugs only intravenously).
It is necessary to hospitalize the patient as soon as possible. Patients with generalized forms of meningococcal infection or with suspicion of them are subject to emergency hospitalization in a specialized department of the infectious diseases hospital by a medical emergency team. If there are signs of ITSH – resuscitation team.
With a progressive worsening of the patient’s condition, hospitalization is shown in the nearest intensive care unit and only after stabilization of the condition is transfer to a specialized hospital.
Mandatory hospitalization are subject to patients with generalized forms of MI or with suspicion of them. On an outpatient basis, only patients with localized forms can be treated: meningococcus and nasopharyngitis with a mild and short course in the absence of preschool children and employees of child care facilities in the family.
- Nasopharyngitis
Antibacterial therapy:
– rifampicin – 10 mg / kg per day for 3-5 days or macrolides (erythromycin, spiramycin, azithromycin), or levomycetin. - Meningococcus
– rifampicin – 2-3 days. - Purulent meningitis
Pre-hospital treatment stage:
– providing venous access;
– antibacterial therapy – chloramphenicol succinate – 25 mg / kg (single dose);
– glucocorticoids – 1-3 mg / kg according to prednisone;
– infusion therapy with saline and colloidal solutions;
– antipyretics;
– furosemide – 1-2 mg / kg;
– with convulsions – diazepam (inpatient treatment phase);
– antibiotic therapy: benzylpenicillin – 300-500 mg / kg administered 6 times a day (reserve antibiotics: ceftriaxone – 100 mg / kg per day, cefotaxime – 200 mg / kg per day; if there are signs of ITS – chloramphenicol succinate – 100 mg / kg per day;
– detoxification therapy for moderate forms using glucose-salt solutions;
– diacarb + aspartame. The dose is selected depending on the severity of the hypertensive syndrome;
– syndromic therapy;
– during convalescence: nootropics, vitamins of group B. - Meningococcemia
Pre-hospital treatment stage:
– providing venous access;
– antibacterial therapy;
– chloramphenicol succinate – 25 mg / kg (single dose) iv;
– glucocorticoids – prednisone, hydrocortisone or dexazone – 2-3 mg / kg for prednisolone – without ITS (in ITS degree 1 – 5 mg / kg, 2nd – 10 mg / kg, 3rd – 15-20 mg / kg);
– infusion therapy with saline or rheopolyglucin to stabilize the bcc;
– inotropes (dopamine) – to maintain hemodynamics (stationary stage of treatment);
– depending on the severity of the condition, the patient is hospitalized in the intensive care and resuscitation department or in the neuroinfection department of the infectious diseases hospital;
– antibiotic therapy: in the presence of ITS, the drug of choice is chloramphenicol succinate at a dose of 100 mg / kg per day (when a patient is withdrawn from ITS, penicillin is prescribed 200 mg / kg per day or cephalosporins 100 mg / kg per day).
In severe form and the need for protection against nosocomial infection, additional use of 3rd generation aminoglycosides – amikacin – up to 20 mg / kg per day, netilmicin – 1.5-2.0 mg / kg every 8 hours;
– detoxification therapy for moderate forms is carried out with glucose-salt solutions, taking into account the daily need for fluid and pathological losses;
– Syndromic therapy – according to the relevant treatment protocols.
Patients are discharged for clinical recovery after normalization of laboratory indicators of cerebrospinal fluid, a general blood test. A control swab from the nasopharynx is taken in a hospital no earlier than three days after antibiotic treatment.
The consequences of generalized forms of meningococcal infection
Clinical and laboratory studies have shown that upon discharge from the hospital, most patients still do not fully recover all the impaired functions. Children who have undergone purulent meningitis must be registered with a neurologist for 2-3 years.
It is advisable not to send children to child care facilities during the first 2-3 weeks after discharge.
The most common consequence of meningococcal infection is cerebrosthenic syndrome, manifested by increased fatigue, sleep disturbance, appetite, decreased performance, and behavior changes. For younger children, emotional instability, motor disinhibition, distracted attention, and sometimes aggressiveness are more characteristic.
When revealing cerebral growth, a child needs to ensure a sparing regimen, the correct organization of work and rest, limiting to a minimum the time of watching TV and working with a computer, increasing the time of sleep and staying in the fresh air, and general strengthening therapy. In the recovery period, nootropics, multivitamins, vascular preparations are prescribed under the control of brain dopplerography.
Prevention of Meningococcal Infection
When a diagnosis of meningococcal infection is established, an emergency notification is sent to each district or city SES. In a children’s institution, quarantine is set for 10 days from the moment of isolation of the last patient. A bacteriological examination (smear from the nasopharynx) is carried out in contact with the carrier at the place of residence and in an institution. Contact children in the institution are monitored: daily examination of the skin, pharyngeal mucosa, thermometry. They are prescribed rifampicin for 2 days at an age-specific dosage.